
Spinal Accessory Nerve Pain
That knot in your trap that never goes away? It might not be your trap at all
You know the spot. The one your partner digs into and you say right there, that's it, and it feels better for about an hour before it's back. The one your remedial massage therapist works on every single session without ever quite resolving it.
Most people call it tight traps or rhomboids. Others get told it's just general tension from stress and posture.
And they're not entirely wrong, those muscles are involved. But in a significant number of cases, the reason that tension never fully resolves, regardless of how much massage, stretching, or manipulation is applied, is that the problem isn't primarily in the muscle at all.
It's a nerve.
The spinal accessory nerve - what it is and why it matters
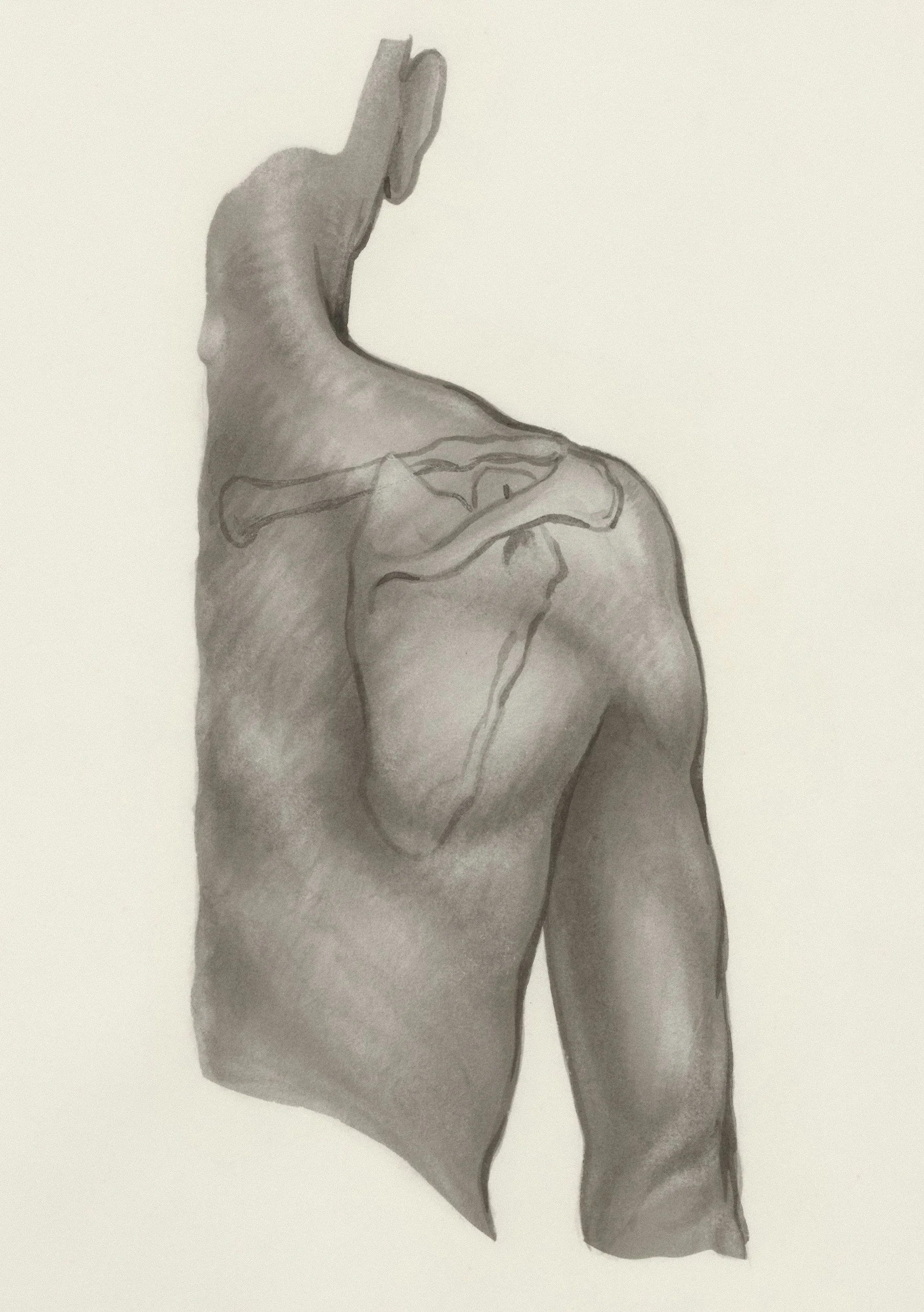
The spinal accessory nerve (cranial nerve XI) is one of the twelve cranial nerves that originate from the brain rather than the spinal cord. It arises from the brainstem, exits the skull, and travels down the back and side of the neck before branching into two main destinations: the sternocleidomastoid muscle at the front of the neck, and the upper trapezius.
It is a purely motor nerve and its job is to control muscle movement, not to carry pain signals. This is part of why it gets overlooked. Most clinicians think about nerve pain in terms of sensory nerves (the ones that produce tingling, radiating pain, or numbness).
“The spinal accessory nerve controls the upper trapezius directly. When this nerve is restricted along its path through the neck, the trapezius muscle it supplies can remain chronically tense and sensitive — regardless of how much soft tissue work is applied to the muscle itself. You can massage a neurally-driven muscle problem all day and produce only temporary relief, because the driver isn’t in the muscle.”
What this actually feels like
The presentation I see consistently in clinic:
A persistent ache or tension in the upper traps - the area between the base of the neck and the top of the shoulder
Pain or sensitivity that runs between the shoulder blades (intrascapular pain)
A specific spot that is often right at the corner where the neck meets the shoulder, or in the mid-trap region between the spine and shoulder blade
Symptoms that ease temporarily with massage or heat but return within hours or a day or two
No lasting change despite repeated adjustments, dry needling, or massage sessions targeting the area
“The phrase I hear more than almost any other: “my rhomboids are so tight”. In many cases when I assess these patients, the rhomboids and mid-trapezius are not the primary problem. The spinal accessory nerve is what’s generating the symptoms. Treating the wrong structure is why the problem doesn’t resolve.”
Who gets this
In short: almost everyone who spends significant time at a desk.
The spinal accessory nerve travels through the neck in a position that is mechanically loaded by sustained forward head posture, the position most people adopt when looking at a screen, reading, studying, or writing. Over time, the chronic irritation and inflammation of the nerve can cause local pain and muscle guarding.
This is not a rare or exotic condition. It is one of the most common presentations I see, it’s so common that targeted assessment of the spinal accessory nerve is now a standard part of how I approach almost every neck and upper back presentation. The reason more people don't know about it is simply that it doesn't have the profile of conditions like a disc herniation or rotator cuff tear. It doesn't show on imaging. It just produces persistent pain and tension that people learn to live with.
Why standard treatment doesn't fix it
Massage applied to the upper trapezius produces relief because it temporarily reduces muscle tension and stimulates blood flow to the area. But if the nerve supplying that muscle is the true cause of their symptoms, the muscle will return to its guarded state relatively quickly. The massage is addressing the consequence, not the cause.
The same principle applies to stretching. You can stretch the upper trapezius and get a brief improvement in range and comfort.
Spinal adjustment is similarly limited here. Cervical and thoracic adjustments can improve joint mobility and reduce pain but an adjustment doesn't specifically address the spinal accessory nerve.
None of this means massage, stretching, or adjustments are wrong or unhelpful. They are part of the picture. But when they're the only tools being used, and the nerve is the primary driver, the relief will always be partial and temporary.
How we approach it at Southside Spine and Sport
Because the underlying issue is a nerve, the treatment needs to be directed specifically at the nerve.
We use targeted soft tissue therapy applied to the spinal accessory nerve, most commonly at the upper trapezius. The technique involves specific contact on the nerve combined with controlled movement that creates a mobilising force along the nerve, breaking any adhesions that may be binding it to the trapezius muscle. The goal is to restore normal nerve mobility and reduce the irritation at adhesion sites that is driving the muscle's chronic guarded state.
This is the same precision approach we use for other nerve entrapment conditions like the cluneal nerve, the sciatic nerve in the deep gluteal region, and the piriformis. The mechanism is the same: find the nerve, find where it's restricted, restore mobility.
Learn more about our soft tissue therapy approach and adhesion release techniques.
“Of all the treatments I apply for neck and upper back pain, spinal accessory nerve work is among the most consistently effective and the most straightforward to apply. If I had to choose just two treatments for a neck presentation without knowing anything else about the patient, this would be one of them alongside the suboccipital muscles. That’s how common and how impactful this nerve is.”
When to seek assessment
If any of the following apply, a clinical assessment is worthwhile:
Persistent upper trap tension or aching that returns within a day or two of massage or treatment
Pain or sensitivity between the shoulder blades that doesn't respond to stretching or adjustment
A specific tender spot at the corner of the neck or in the mid-trap region that you've been managing for months or years
Neck stiffness or restricted rotation alongside upper back tightness
You've been told it's your rhomboids or mid-traps and treatment targeting those areas isn't producing lasting change
“The following symptoms alongside neck and upper back pain warrant
prompt medical assessment rather than chiropractic care as a first step:
- Significant arm weakness or hand clumsiness that has developed
recently
- Unexplained weight loss alongside neck or upper back pain
- Symptoms that are rapidly and progressively worsening”
Frequently asked questions
What is the spinal accessory nerve?
The spinal accessory nerve (cranial nerve XI) originates from the brainstem and travels down the back of the neck, supplying the upper trapezius and sternocleidomastoid muscles. It is a purely motor nerve which means it controls muscle movement. It is frequently overlooked as a contributor to persistent upper back, neck, and intrascapular pain.
Can the spinal accessory nerve cause upper back and trap pain?
Yes. When the spinal accessory nerve is irritated, the trapezius muscle it supplies can remain chronically tense and painful regardless of how much soft tissue work is applied to the muscle itself. Addressing the nerve directly is often what produces lasting change when other treatments have provided only temporary relief.
Why do my traps feel permanently tight no matter what I do?
Persistent trap tightness that doesn't respond to massage, stretching, or spinal adjustment is often being driven by something other than the muscle. The spinal accessory nerve is a frequently missed contributor. When this nerve is irritated or trapped, the muscle it supplies remains in a chronically guarded state regardless of how much treatment is directed at the muscle.
What is intrascapular pain?
Intrascapular pain is pain felt between the shoulder blades. It is commonly attributed to tight rhomboids or mid- trapezius muscles, and while these can be involved, persistent intrascapular pain that doesn't respond to treatment of those muscles is often being driven by the spinal accessory nerve or other cervical nerve structures rather than the muscles themselves.
How is spinal accessory nerve dysfunction treated?
We use targeted soft tissue therapy directed at the spinal accessory nerve, usually at the upper trapezius, aiming to restore normal nerve mobility and reduce irritation at sites where the nerve may be adhered or trapped. This is distinct from general trap massage and targets the nerve rather than the muscle. Results are assessed at each visit and treatment is adjusted accordingly.
Persistent upper trap tension or mid-back pain that treatment hasn't been able to shift?
A proper clinical assessment will identify whether the spinal accessory nerve is a contributing factor and give you a clear path forward.
Book an appointment online or send us a message if you'd prefer to ask a question first.
We're based in Bicton and see patients from across Perth's southern suburbs, including Fremantle, Melville, East Fremantle, Cockburn, and surrounding areas.