
What is Shoulder Bursitis and Shoulder Impingement
WRITTEN BY DR RUSSELL JENSEN
Principal Chiropractor Southside Spine and Sport, Bicton WA
AHPRA Registration: CHI0001927257 Practising chiropractor since 2015.
Trained in Integrative Diagnosis (USA).
Special interest in shoulder injuries, nerve pain, and sports rehabilitation.
→ Full profile: southsidespinesport.com.au/meet-our-chiro

What is shoulder bursitis and shoulder impingement?
Every summer in Perth — and again around the silly season — we see a reliable wave of patients with shoulder pain. People come out of a quieter winter, pick up the pace, and something that's been a minor background issue becomes a genuine problem. If the pain you're experiencing is worse when lifting your arm, reaching overhead, or lying on that side at night, shoulder bursitis or impingement are worth understanding.
In this article I'll explain what these two conditions are, how they're related, what you can do at home right now, and what to expect from professional treatment. I'll also explain where we sit in the treatment hierarchy — because knowing your options makes it easier to choose the right path.
What is shoulder bursitis?
Shoulder bursitis is inflammation of the bursa — a small fluid-filled sac that sits above the rotator cuff tendons, between them and a bone called the acromion. When it's healthy, the bursa is as thin as tissue paper and acts as a friction-reducer, allowing smooth movement between these structures.
When the bursa becomes inflamed — usually from overuse, repetitive overhead movement, or a sudden spike in loading — it swells. A swollen bursa takes up space that wasn't designed to accommodate it, and the result is pain, particularly when lifting the arm to the side or overhead.
“In plain terms: bursitis is inflammation of a cushioning sac in the shoulder. The bursa’s job is to stop things from rubbing. When it swells, it becomes part of the problem instead of the solution.”
What is shoulder impingement?
Shoulder impingement occurs when the supraspinatus tendon — part of the rotator cuff — gets pinched between the ball of the shoulder joint and the acromion bone above it when you lift your arm.
The hallmark sign is what clinicians call a "painful arc." Pain appears as you raise your arm to roughly 60–120 degrees, then often eases above that range as the pinching resolves. If this sounds familiar — raising your arm to shoulder height hurts, but reaching fully overhead is actually less painful — that pattern is highly suggestive of impingement.
“Bursitis and impingement very commonly occur together. Impingement is the mechanical cause — the tendon getting pinched. Bursitis is the inflammatory consequence — the bursa reacting to being repeatedly compressed. Treating one without addressing the other is one of the most common reasons people don’t fully recover.”
What causes these conditions?
The most common cause is a sudden increase in activity the shoulder isn't conditioned for — starting a new gym program, returning to swimming after winter, painting ceilings, or increasing workload in a physically demanding job.
Underlying factors that make the shoulder more susceptible include:
Weakness in the external rotator muscles of the shoulder, which are responsible for stabilising the ball of the joint and preventing impingement during arm movement
Poor scapular (shoulder blade) control, which affects the angle of the acromion and how much space the rotator cuff has to work in
Postural patterns that encourage the shoulder to sit forward, reducing the subacromial space
Previous shoulder injury that hasn't been fully rehabilitated
The good news is that all of these are addressable. The shoulder responds well to targeted strengthening, and this is the part of recovery that creates lasting change rather than temporary relief.
When should I see a professional?
The following symptoms alongside shoulder pain may indicate something more serious than bursitis or impingement. See a doctor promptly if you experience:
Significant shoulder weakness — not just pain with movement, but genuine inability to raise the arm
Pain that came on after a fall or direct trauma to the shoulder (possible fracture or rotator cuff tear)
Severe swelling, heat, or redness around the joint (possible infection or inflammatory arthritis)
Symptoms that are rapidly worsening rather than fluctuating
Pain radiating down the arm toward the hand, especially with numbness or tingling (possible nerve involvement — see our page on nerve pain
If none of these apply, there's no need to panic — but getting a professional assessment before starting any exercise program is always the right first step.
What can you do at home right now?
Many people can make meaningful progress with home exercises while they wait for a professional appointment, or alongside treatment. The key rule: exercises must be pain-free. Working through mild resistance or muscle fatigue is fine. Working through actual pain is not — it feeds the inflammatory cycle.
The three exercises we give to every shoulder patient at our clinic to build a strong foundation for recovery:
1. Depth push-ups or dips

These are performed with a larger range of motion than a standard push-up or dip — going deeper than you normally would. The goal is to expose the shoulder to the end-ranges of movement in a loaded but controlled way. This stimulates the connective tissue and rotator cuff in the positions they're most often neglected.
If push-ups are too difficult initially, start against a wall or an elevated surface. Depth dips can be done on the edge of a chair.
2. Seated external rotation

The external rotators of the shoulder — particularly the infraspinatus and teres minor — perform the critical job of stabilising the humeral head and decelerating arm movement. In most people with shoulder impingement, these muscles are undertrained relative to the internal rotators.
You can do this exercise seated on a chair or lying on the floor. Hold a light weight — a water-filled bottle works perfectly — and rotate the forearm outward from a 90-degree elbow position. The movement is small and controlled. No swinging.
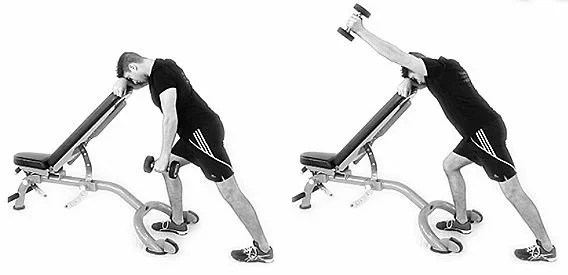
3. Trap 3 raise
The lower trapezius is essential for healthy scapular rotation — it tilts the shoulder blade upward when you lift your arm, which opens the subacromial space and reduces impingement. In most people with shoulder problems, it's inhibited and underworking.
The Trap 3 raise can be done one arm at a time, leaning forward at roughly 45 degrees and raising the arm diagonally away from the body. A light weight or no weight at all is sufficient to start. If you have a workout bench, use it — but leaning on a kitchen bench, a car bonnet, or any stable surface works just as well.
What professional treatment options are there?
Conservative management (our starting point)
For the majority of people, conservative management resolves shoulder bursitis and impingement without any injections or surgery. This combines hands-on treatment to improve range of motion, reduce pain, and identify the specific movement deficits contributing to the problem, alongside a progressive home exercise program.
At Southside Spine and Sport, every shoulder patient begins with a full assessment and manual treatment. After one or two sessions, when pain has reduced and movement has improved, we introduce the exercises above. Most patients do them once a day — they take about ten minutes. See our rehabilitative exercises page for more on how we approach exercise-based recovery.
Shockwave therapy
Shockwave therapy delivers acoustic energy pulses to the affected tissue, stimulating a healing response in chronically inflamed tendons and bursae and reducing pain sensitisation. It is particularly effective for cases that haven't responded to conventional treatment alone — including calcific tendinopathy, which is a specific type of shoulder impingement where calcium deposits form in the tendon.
Learn more about our shockwave therapy service.
“At most clinics, shockwave therapy is charged as an additional fee on top of the consultation — typically $50–$80 extra per session. At Southside Spine and Sport, shockwave is included in our standard consultation fee at no extra cost. We include it because we believe it should be available to every patient who can benefit from it, not just those who can afford the premium.”
Steroid injection
Steroid injections are sometimes recommended when pain is severe enough to prevent participation in rehabilitation. They are most effective when given under ultrasound guidance to ensure accurate placement. The injection reduces inflammation and buys a window of reduced pain — but this must be used to do the rehabilitation work, not as a standalone solution.
Subsequent injections carry an increasing risk of tendon damage. If you are considering a steroid injection, it is worth exhausting conservative options — including shockwave — first.
Surgery
Surgery is reserved for cases where conservative management has genuinely failed — typically after six or more months of properly applied treatment. It is sometimes necessary, and we will always support you in getting the right referral when that's the appropriate next step. We can provide a detailed letter to your GP summarising what we've tried and what the outcome has been, which makes the referral process faster.
How long does recovery take?
Most people with shoulder bursitis or impingement see meaningful improvement within 6–12 weeks of consistent treatment and exercise. What drives the variability is rarely the condition itself — it's consistency with the rehabilitation and whether the underlying movement deficits have been properly addressed.
Full recovery, including a confident return to overhead sport, swimming, or heavy gym work, typically takes 3–6 months. This sounds long, but the strengthening phase is cumulative — each week builds on the last, and most people feel functional well before they reach the endpoint of rehabilitation.
Frequently asked questions
What is the difference between bursitis and impingement?
Bursitis is inflammation of the bursa — the fluid-filled cushioning sac in the shoulder. Impingement is the mechanical pinching of the rotator cuff tendon under the acromion bone. They are technically distinct but very frequently occur together, because repeated impingement of the tendon also compresses the bursa. Most patients have elements of both.
Can I exercise with shoulder bursitis?
Yes, but with modification. High-overhead movements, behind-the-neck pressing, and anything that provokes the painful arc should be avoided until symptoms settle. The exercises described in this article are designed to be done during the recovery phase. Pain is the guide — if an exercise causes it, stop and seek advice before continuing.
Is shoulder bursitis the same as a rotator cuff tear?
No. Bursitis is inflammation of the bursa; a rotator cuff tear is a partial or full rupture of one of the rotator cuff tendons. They can produce similar symptoms, which is why a proper clinical assessment — and sometimes imaging — is important. Tears typically involve more noticeable weakness and may not respond as well to conservative care.
How long does shoulder bursitis take to heal?
With appropriate conservative treatment, most people see meaningful improvement within 6–12 weeks. Full recovery including return to sport or heavy lifting is typically 3–6 months. Shockwave therapy can accelerate the process, particularly for chronic or calcific cases.
Can shoulder bursitis be treated without surgery?
Yes — the majority of cases resolve without surgery. Conservative management including manual therapy, progressive exercise, and shockwave therapy is effective for most people. Surgery is a last resort, recommended only when conservative management has failed after 6+ months.
What exercises help shoulder bursitis and impingement?
The three exercises we recommend for all shoulder patients are depth push-ups or dips, seated external rotation, and the Trap 3 raise. These address the most common underlying deficits: lack of full-range loading, external rotator weakness, and poor lower trapezius activation. They can all be done at home with no or minimal equipment.
If you're dealing with shoulder pain that isn't improving on its own, we'd be glad to help. A proper assessment will tell you exactly what's going on and give you a clear path forward.
Book an appointment online or send us a message if you have a question first.
We're based in Bicton and see patients from across Perth's southern suburbs, including Fremantle, Melville, East Fremantle, Cockburn, and the surrounding areas.
Reviewed and updated by Dr Russell Jensen, Principal Chiropractor (AHPRA: CHI0001927257), Southside Spine and Sport - May 2026. Originally published December 2023.
This article is for general information only and does not constitute medical advice. Always consult a qualified health professional for diagnosis and treatment of shoulder pain.